Gair, Gair, Conason, Rubinowitz, Bloom, Hershenhorn, Steigman & Mackauf Home
Gair, Gair, Conason, Rubinowitz, Bloom, Hershenhorn, Steigman & Mackauf HomeFailure to Diagnose Abdominal Compartment Syndrome Attorney
The New York City Medical Malpractice Attorneys at Gair, Gair, Conason, Rubinowitz, Bloom, Hershenhorn, Steigman & Mackauf represent victims of Abdominal Compartment Syndrome Misdiagnosis. Contact us at 212-943-1090 for a free consultation.
Abdominal Compartment Syndrome (ACS) is a life-threatening condition that occurs when pressure builds up within the abdominal cavity, restricting blood flow to vital organs. Left untreated, it can lead to multiple organ failure and death.
The condition often develops after trauma, abdominal surgery, pancreatitis, or severe infection. Diagnosis requires close monitoring of intra-abdominal pressure, as symptoms may be nonspecific and easily overlooked. Rapid recognition and emergency intervention—often surgical decompression—is critical to survival.
When a physician fails to recognize or timely diagnose ACS, patients may suffer catastrophic injuries such as kidney failure, respiratory distress, bowel ischemia, or cardiac arrest.
- Ignoring obvious symptoms such as severe abdominal distention, decreased urine output, or respiratory compromise.
- Failure to monitor intra-abdominal pressure in high-risk patients following surgery or trauma.
- Misdiagnosis of ACS as another condition, leading to dangerous delays in treatment.
- Failure to order emergency surgery when signs of organ dysfunction appear.
- Medical expenses, including future care needs
- Loss of income and reduced earning capacity
- Pain and suffering
- Wrongful death damages for surviving family members
For over a century, our firm has been at the forefront of complex medical malpractice litigation in New York. Our attorneys have obtained some of the largest verdicts and settlements in New York Sate and nationaly, including record-breaking results in failure to diagnose and surgical error cases.
What sets us apart:- Decades of experience handling highly complex medical malpractice cases.
- Access to top medical experts who can explain how the standard of care was breached.
- Proven trial lawyers who are respected—and feared—by defense attorneys and insurance companies.
- A track record of recovering multi-million-dollar verdicts and settlements for patients and their families.
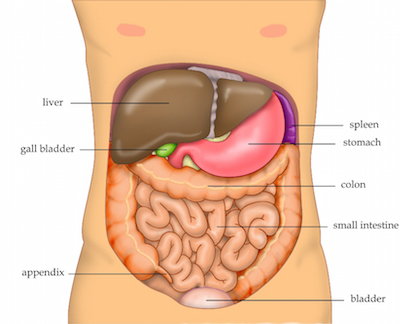
Compartment Syndrome occurs when the pressure within a closed anatomic space (a compartment) becomes so elevated that capillary perfusion is compromised. Any closed anatomic space including the abdominal cavity is at risk of developing a compartment syndrome. Abdominal compartment syndrome is a clinical disease spectrum that results from increased intra-abdominal pressure (IAP) due to tissue edema or free fluid collecting in the abdominal cavity. Elevated pressure in the abdomen is referred to as intra-abdominal hypertension (IAH). Abdominal compartment syndrome is the end stage organ failure that occurs due to the pathophsiologic derangements that occur as a result of increasing intra-abdominal pressure. The end stage of undetected and untreated intra-abdominal hypertension is multi-system organ failure and patient death. 1
Intra-abdominal hypertension (IAH) is defined as the sustained or repeated pathologic elevation of intra-abdominal pressure (IAP) greater than or equal to 12 mmHG. Abdominal compartment syndrome is defined as a sustained IAP greater than 20 mmHG that is associated with the development of new organ dysfunction or failure. 2
Elevated intra-abdominal pressure can cause significant impairment of cardiac, pulmonary, renal, gastrointestinal, hepatic and central nervous function. The effects of IAH are not just limited to the intra-abdominal organs, but rather have an impact on every organ system in the body. 3
The sensitivity of both clinical judgment and physical examination have been demonstrated to be very poor in predicting a patient’s IAP. Early serial IAP measurements are therefore essential to both diagnosing the presence of IAH as well as guiding resuscitative therapy. While a variety of methods for IAP measurement have been described, intra-vesicular or bladder pressure has achieved the most widespread adoption worldwide due to its simplicity, minimal cost and low risk complications. Prolonged elevations in IAP’s of 10-20 mmHG can result in organ dysfunction and failure while pressures above 25mmHG are associated with potential mortality. 4
Immediate abdominal decompression should be performed in any patient who demonstrates significant elevations in IAP or evidence of ACS. In surgical patients, this is best achieved by either creating or reopening their laparotomy incision and applying a temporary abdominal closure. 5
Elevated IAP causes significant impairment of cardiac, pulmonary, renal, gastrointestinal and hepatic function with each organ demonstrating its own unique vulnerability. 6
Accurate and timely assessment of intra-abdominal pressure is crucial to the diagnosis and management of both intra-abdominal hypertension and abdominal compartment syndrome. As elevated IAP may occur insidiously and clinical examination is notoriously inaccurate in determining the presence of IAH, IAP measurements are an indispensable tool in the modern intensive care unit (ICU) setting. 7
Abdominal compartment syndrome is well recognized as a potential complication of laparotomy for trauma. It has also been reported after repair of large ventral hernias and may be anticipated in any case in which there is a loss of domain for abdominal organs. 8
Failure to diagnose Intra-Abdominal Hypertension leading to Abdominal Compartment Syndrome, multi-system organ failure and patient death following surgery of the Abdominal Cavity may constitute medical malpractice.
Read more about Medical Malpractice Relating to Failure to Diagnose Compartment Syndrome of the Lower Leg.
-
Overview: Intra-abdominal hypertension and abdominal compartment syndrome www.abdominal-compartment-syndrome.org/IAH
-
Cheatham ML, DeWaele JJ, Kirkpatrick A, et. al. Criteria for a diagnosis of abdominal compartment syndrome. Can J. Surg 2009; 52(4): 315-316
-
Cheatham ML, Abdominal Compartment Syndrome: pathophysiology and definitions. Scand J Trauma Resusc Emerg Med. 209; 17:10
-
id.
-
Ivatury RR, Cheatham ML, Malbrain MLNG, Surgue, M, editors, Abdominal Compartment Syndrome. Georgetown: Landes Biosciences; 2006.
-
id.
-
id.
-
Dalencourt G, Katlic MR. Abdominal compartment syndrome after late repair of Bochdalek Hernia. Ann Thosac Surg 2006; 82: 721-2
Contact Gair, Gair, Conason, Rubinowitz, Bloom, Hershenhorn, Steigman & Mackauf at 212-943-1090 or fill out our online form to schedule a free consultation.
Disclaimer: Please be advised that the results achieved in any given case depend upon the exact facts and circumstances of that case. Gair, Gair, Conason, Rubinowitz, Bloom, Hershenhorn, Steigman & Mackauf cannot guarantee a specific result in any legal matter. Any testimonial or case result listed on this site is based on an actual legal case and represents the results achieved in that particular case, and does not constitute a guarantee, warranty or prediction of the outcome of any other legal matter.